




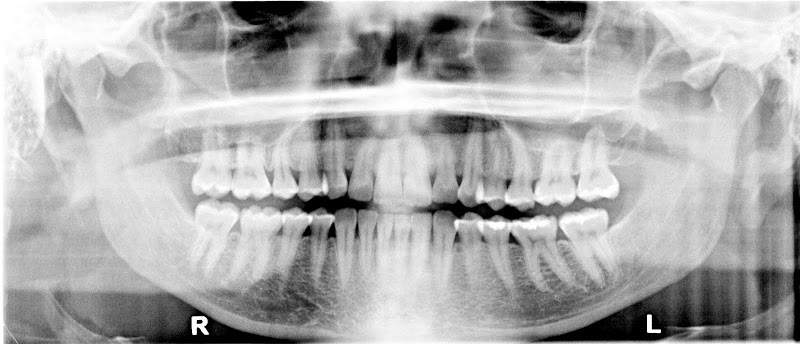
On the left side, teeth #11 and #12 have a notched abfraction and strong recession. The right side shows recession on #3, #4, #5, and #30. This is a maxilla to mandible skeletal asymmetry case that has had a lifetime of sinus issues. The upper arch is the shape of a “V” and the mandible has a “U” shape. A “U” does not fit inside of a “V” so the force scans will find the unbalanced pattern.
Notice the full face picture and how the labial fold is different on the left versus the right. This is diagnostic to what we see inside the mouth. Her left maxilla is narrow and not symmetrical to the right maxilla. The midline of the centrals is left of center and the periodontal tissue change at the distal of #9 and do not return to normal until tooth #13. Many patients have periodontal changes as a result of a skeletal growth asymmetry in growth. Chronic allergies as a child had a strong influence on vaulting the palate. The maxilla has a “V” shape as a result and the mandible grew in a more normal “U” shape.
The Habitual pattern shows that the patient chews away from the the left corner.
FUNCTION HEALTH
The patient has had issues with her jaw and neck that started with a 1995 auto accident. Patient states “I have had TMJ since 1995 and my jaw is constantly moving. What can I do?” A California dentist made a lower splint in 1995 that was worn for 5 years. The narrow growth pattern of the maxillary bones are more than likely due to childhood allergies. Functionally speaking, the bones and the teeth are not aligned well for optimum function. The teeth are in good condition, so the periodontal and referring pain patterns are the primary concern.
FUTURE CONSIDERATIONS…
The key to this case is building trust. A full upper splint at night to start, followed by physical therapy for the neck and shoulders. Equilibration or orthodontics will be required in the future to neutralize the wedge effect on the teeth.